Figure 1
Objective career development. Distribution of the objective career development sum score (percentage of participants), defined on objective criteria for academic success (Career development sum score) with a range from 0 to 11.
DOI: https://doi.org/10.4414/smw.2011.13233
Mentorship is a type of formal social support and has been highlighted as a vital component for personal and career advancement, research productivity, career selection and interest in academic medicine [1, 2]. Congruously, a lack of mentoring is among the main reason for a deficiency in career success in academic medicine, especially for women [2–7]. The concept of mentoring was described in the late 1970s by Levinson [8], who revealed the mentoring relationship to be one of the most important factors an individual can have in early adulthood, and was continued by several others in the 1990s when establishing formal mentoring programmes [9, 10]. Increasing administrative tasks, clinical challenges (e.g. work hour limitations, availability of residents) and research duties hamper the constitution of mentor-mentee relationships [2]. Moreover, it has been reported that female physicians working in university or county hospitals receive less support than male physicians, and mentoring experiences in these hospitals are significantly worse in “surgical fields” compared to “internal medicine” [11].
The gender gap that existed in the composition of medical students in Western countries for a very long time is now essentially closed [12]. For instance, since 2005 more than half of the medical school graduates in Switzerland were women; indeed, in 2008/2009 there were 62.1% [13]. In contrast and comparable to other European countries, only 9.6% of the general surgeons in 2008 were women [14–16]. Overall, about 10% of the young physicians in Switzerland aspire to have an academic career, although female physicians generally show less interest in academic pursuits than men [17–19]. Similarly, they have lower objective career success in terms of publications, grants, scholarships and research activities [17, 18, 20].
In the early stages of specialty training, a larger fraction of residents contemplate pursuing an academic career with an equal distribution between the sexes [20]. Possible reasons for this decrease are, on one hand, the need for hard work and perseverance for a successful career in academic surgery [21].
On the other hand, a lack of a mentor-mentee relationships, role models and career guidance can be limiting factors as they are crucial pre-requisites on the way to becoming an academic surgeon [20]. Only few women are willing to prioritise their professional career at the expense of their personal life [22, 23]. A reason for the incompatibility of work and family life are rigid career paths [19, 24]. However, the personal situation often has an influence on the choice of career path and success in terms of receiving support from a partner and of the amount of housework obligations [25]. Female physicians with children often work reduced hours and abstain from an academic career, mainly to enable them to fulfil family commitments [26]. This also applies to their specialty choice: female physicians are significantly under-represented in prestigious surgical specialties [24, 27, 28].
In a previous study, we showed the factors influencing the choice of a career in surgery in Switzerland and how the appeal of the specialty could be improved [29]. In the near future, there might be not only a lack of surgeons in some Western countries including Switzerland, but especially also of young academics. The aim of the present study was to analyse factors critical for a successful academic career for female surgeons in Switzerland and to assess the value of a mentor-mentee relationship in this context.
This study was based on an anonymous national survey of female board-certified surgeons in Switzerland. They were identified from the database of the Swiss Surgical Society (2008: 1178 members, including 94 women). Furthermore, female surgical residents participating at the annual congresses 2006/2007 of the Swiss Surgical Society were approached. Data were collected during spring 2008. Response enhancement techniques included advance notification and a mailed reminder.
To ensure the participants’ anonymity, returned questionnaires were identified only by a code, and participants sent their responses to an independent administration office allowing for further queries. The Cantonal Ethical Committee of Graubunden ruled that this study did not require ethical approval.
The questionnaire included 4 parts. Part 1 addressed sociodemographic data (age, marital status, number of children, professional status, field of work and career aspiration).
In part 2, the respondents were asked about the presence of mentor-mentee relationships (yes/no) and success regarding career advancement and career satisfaction in general, scored on a seven-point Likert scale (1 = “very dissatisfied” to 7 = “very satisfied”).
Part 3 of the survey consisted of 16 items regarding the support in career advancement. A subdivision into five scales (networking, career planning, coaching, role model and emotional support scale) was performed according to the “Mentoring Function Items” of Noe and the “Career support scale” of Riley and Wrench [30, 31]. Each item was rated on a five-point Likert scale, scored by 1 = strongly disagree and 5 = strongly agree. To facilitate the interpretation of the results, answers were dichotomised (1 to 3 vs. 4 and 5) for the multivariate analysis.
Part 4 was based on questions about the planning and development of the participants’ professional career. Career development was assessed using objective criteria [32–35]: “talks at conferences”, “number of publications”, “participation in research projects”, “months of research as a fulltime activity”, “scholarships awarded”, “third-party funds” and “number of research awards obtained”. The items were summarised to obtain a comparable value for career success with a range from 0 to 11 (table 1). This sum score has been validated by Buddeberg et al. in terms of career choice and essential test-statistical criteria [17].
Continuous data were expressed as medians (range), and dichotomous data were expressed as frequencies and percentages. The Mann-Whitney U test was used to compare continuous variables. Dichotomous and categorical outcomes were analysed using Fisher’s exact test. A logistic regression multivariate analysis was performed to evaluate the effect of having a mentor. Collected data were analysed by using SPSS version 13.0 (SPSS; Chicago, Illinois, USA). All statistical tests were two-sided with a significance level of 0.05.
| Table 1: Objective factors for career development in 189 female surgeons and residents [32–35]. | ||
| Objective factor | Item value for the career development sum score | Value |
| Talks at scientific conferences, median (range) | No talk = 0 1–3 talks = 1 ≥4 talks = 2 | 1 (0–52) |
| Number of publications in a peer-reviewed journal, median (range) | No publication = 0 1 publication = 1 2–3 publications = 2 ≥4 publications = 3 | 0 (0–35) |
| Current participation in any research project, No. (%) | No = 0, yes = 1 | 34 (18) |
| Fulltime research activity, median (range), months | No = 0 ≤9 months = 1 >9 months = 2 | 0 (0–24) |
| Scholarship awarded, No. (%) | No = 0, yes = 1 | 11 (6) |
| Third-party fund awarded, No. (%) | No = 0, yes = 1 | 16 (9) |
| Research awards obtained, No. (%) | No = 0, yes = 1 | 33 (18) |
| Career development sum score, median (range) | 0–11 | 2 (0–11) |
Of 318 surveys mailed, there were 189 responses (response rate of 59.4%). Replies were received from 106 (56%) residents and 83 (44%) board-certified surgeons (table 2).
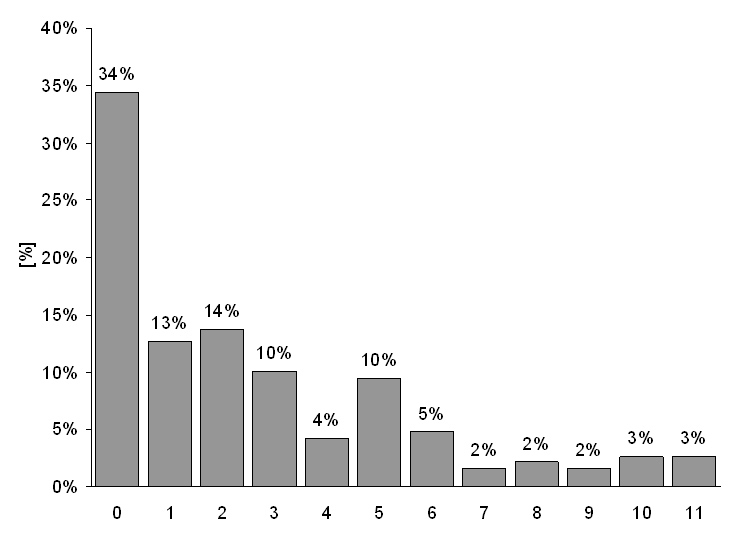
Figure 1
Objective career development. Distribution of the objective career development sum score (percentage of participants), defined on objective criteria for academic success (Career development sum score) with a range from 0 to 11.
The median age of the respondents in the survey was 33 (range 25–63) years. The majority of participants (166/188; 88%) worked in a surgical field, whereas 6 (3%) female board-certified surgeons were employed in a non-surgical field and 16 (9%) indicated family duties as their field of work. As a career choice, 111/189 (59%) indicated a clinical, non-academic career in a hospital, 37 (20%) sought a clinical, non-academic career in a private practice, and 17 (9%) aimed for an academic career.
Overall, 140/189 (74%) were married or living with a partner, and 53/140 (38%) of the partners were physicians, as well. A family with at least one child was reported by 46 (24%) participants, and 51 (27%) women did 100% of the housework themselves. Participants with children were significantly older (39.5, range 27–63 years) than those without children (31, range 25–63 years) (p <0.01).
Mentor-mentee relationships were reported by 109/189 (58%) respondents. Mentorships existed in 62 of 106 (58%) residents and 47 of 83 (57%) surgeons (p = 0.88). Table 3 shows the mentors’ characteristics.
The support of the respondents‘ career advancement by their work environment was evaluated based on 16 items (table 4) [30, 31]. Mentoring significantly enhanced the support in professional advancement, especially in terms of networking and career planning (table 4).
Of all respondents with mentors, only 3/109 (3%) evaluated the mentor-mentee relationship as not helpful. Although the satisfaction with career advancement was significantly higher in women with a mentor-mentee relationship (4.5 ± 1.7 vs. 3.5 ± 1.4; p <0.01), the presence of a mentor did not have an influence on choosing an academic career (11/109 (10%) vs. 6/80 (8%); p = 0.27). Structured (13/109, 12%) compared to non-structured mentoring programmes (96/109, 88%) did not improve satisfaction (4.5 ± 1.3 vs. 4.5 ± 1.7; p= 0.93).
There was a trend to have more publications in respondents with a mentor-mentee relationship (1 (0–35) vs. 0 (0–31); p = 0.06), however, the likelihood of completing the doctoral thesis was similar (76/109 (70%) vs. 60/80 (75%); p = 0.43).
The mentor’s sex did neither have a significant effect in terms of rating the relationship as helpful (81/92 (88%) for male vs. 14/17 (82%) for female mentors; p = 0.58) nor in terms of satisfaction with the support in professional advancement rated on a seven-point Likert scale (4.6 ± 1.7 for male vs. 4.0 ± 1.6 for female mentors; p = 0.68).
The distribution of the career development sum score is shown in figure 1. Of all respondents, 65 (34%) had a sum score of 0 with a sloping number of participants towards higher sum scores and a median value of 2 (range 0–11). Only 12 % of the respondents had a career development sum score of 6 or more. Overall, 66/189 (35%) did not give any talks at conferences, 103/189 (54%) of the participants had not published, and 161/189 (85%) had not had any research activity in the past.
Participants aspiring to have an academic career had the highest median sum score (10, range 3–11), followed by those aspiring to have a non-academic hospital career (2, range 0–10) and intending to work in a private practice (1, range 0–8) (table 5). The sum score of respondents who intended to start an academic career or aspiring not to open a private practice was significantly higher (p <0.01 and p = 0.03, respectively). In the bivariate analysis, there was a trend towards a higher sum score in respondents with children (p = 0.09), who had support in doing the housework (p = 0.09) and who were in a mentor-mentee relationship (p = 0.09) (table 6).
The career development sum score of board-certified surgeons (2, range 0–11) was significantly higher than the score of residents (1, range 0–10) (p<0.01), even though the difference seems to be very small. We could not find a significant difference in the career development sum score between participants working in surgery (2, range 0–11) and in a non-surgical field (non-surgery or family duties as a full-time occupation) (2, range 0–11; p = 0.88).
| Table 2: Respondents’ characteristics. | |
| Characteristic | Value (n = 189) |
| Professional status, No. (%) | |
| Surgical Residents | 106 (56) |
| Board-certified Surgeons | 83 (44) |
| Age, median (range), y | 33 (25–63) |
| Time since state examination, median (range), y | 6 (1–37) |
| Full-time activity, No. (%) | 156 (83) |
| Present field of work, No. (%), 1 missing value | |
| Surgery | 166 (88) |
| Non-surgery (e.g. administration) | 6 (3) |
| Family duties as full-time occupation | 16 (9) |
| Career aspiration, No. (%) | |
| Hospital career | 111 (59) |
| Private practice | 37 (20) |
| Academic career | 17 (9) |
| Others / not specified | 24 (13) |
| Existence of a mentor-mentee relationship, No. (%) | 109 (58) |
| Married or with a partner, No. (%) | 140 (74) |
| ≥1 Children, No. (%) | 46 (24) |
| Table 3: Characteristics of mentor-mentee relationships. | |
| Characteristic | Value |
| Existence of a mentor-mentee relationship, No. (%) | 109 (58) |
| Age of mentor, median (range), y | 45 (31-70) |
| Mentors’ sex, No. (%) | |
| Female | 17 (16) |
| Male | 92 (84) |
| Mentors’ area of work, No. (%) | |
| Hospital | 101 (93) |
| Private practice | 6 (6) |
| Research | 1 (1) |
| Unknown | 1 (1) |
| Mentors’ hierarchical position, No. (%) | |
| Head of department at a university hospital | 10 (9) |
| Head of department at a non-university hospital | 38 (35) |
| Specialist Registrar | 55 (50) |
| Specialist in private practice | 6 (6) |
| Table 4: Multivariate analysis of the support in career advancement [1, 2]. | |||||
| Characteristic | n = 189 | without mentor n = 80 | with mentor n = 109 | p | OR (95% CI) |
| Networking scale There are persons in my professional environment who… | |||||
| 1. promote contact with important superiors | 65 (36%) | 14 (18%) | 51 (48%) | <0.01 | 4.11 (2.05–8.22) |
| 2. promote contact with persons who have a positive effect on my career | 70 (38%) | 15 (19%) | 55 (51%) | <0.01 | 4.36 (2.21–8.58) |
| 3. help me prepare for a promotion | 81 (44%) | 23 (29%) | 58 (54%) | <0.01 | 2.83 (1.53–5.25) |
| 4. help me to promote my career by their influence | 72 (39%) | 20 (26%) | 52 (48%) | <0.01 | 2.69 (1.43–5.07) |
| Career planning scale There are persons in my professional environment who… | |||||
| 5. help me with career planning | 75 (40%) | 16 (20%) | 59 (55%) | <0.01 | 4.74 (2.43–9.24) |
| 6. give me tips for my professional future | 108 (58%) | 29 (37%) | 79 (73%) | <0.01 | 4.70 (2.51–8.77) |
| 7. encourage me to take charge of my surgical career | 97 (52%) | 23 (29%) | 74 (69%) | <0.01 | 5.20 (2.76–9.81) |
| Coaching scale There are persons in my professional environment who… | |||||
| 8. help me to learn the technical aspects of my work | 115 (62%) | 41 (53%) | 74 (69%) | 0.03 | 1.96 (1.08–3.59) |
| 9. often give me good technical advice | 127 (68%) | 45 (57%) | 82 (76%) | 0.01 | 2.38 (1.27–4.46) |
| Role model scale There are persons in my professional environment who… | |||||
| 10. I try to copy with regard to their surgical techniques and strategies | 113 (61%) | 42 (54%) | 71 (66%) | 0.09 | 1.69 (0.93–3.08) |
| 11. are role models to me | 89 (48%) | 37 (47%) | 52 (49%) | 0.88 | 1.05 (0.58–1.88) |
| 12. have qualities, which I would like to adopt for myself | 127 (68%) | 54 (68%) | 73 (68%) | 0.99 | 0.99 (0.53–1.86) |
| Emotional support scale There are persons in my professional environment who… | |||||
| 13. listen to me when I talk about my concerns and feelings | 68 (37%) | 22 (28%) | 46 (43%) | 0.03 | 1.95 (1.05–3.64) |
| 14. support me emotionally and encourage me during stressful times | 69 (37%) | 25 (32%) | 44 (41%) | 0.20 | 1.49 (0.81–2.73) |
| 15. take a real interest in my personal advancement | 71 (38%) | 18 (23%) | 53 (49%) | <0.01 | 3.27 (1.71–6.24) |
| 16. are kind to me | 51 (27%) | 17 (22%) | 34 (31%) | 0.13 | 1.68 (0.85–3.28) |
| OR = odds ratio; CI = confidence interval. Evaluation of the support in career advancement based on 16 items, subdivided into five scales. Answers were collected based on a five-point Likert scale: (1 = strongly disagree, 2 = disagree, 3 = neither agree nor disagree, 4 = agree, 5 = strongly agree). The statistical analysis refers to a binary classification of the sum of 4 and 5 vs. 1, 2 and 3 (depicted is the sum of 4 and 5). Depending on the presence of a mentor, the participants were divided into two subgroups. The p value and OR were calculated in terms of presence versus absence of a mentor. | |||||
| Table 5: Career development sum scores of different career aspirations. | |||
| Career aspiration | Career development sum score | p Value | |
| Hospital career | No | 2 (0–11) | 0.50 |
| Yes | 2 (0–10) | ||
| Private practice | No | 2 (0–11) | 0.03 |
| Yes | 1 (0–8) | ||
| Academic career | No | 1 (0–10) | <0.01 |
| Yes | 10 (3–11) | ||
| Values are median (range). | |||
| Table 6: Differences in the value of the objective career development depending on different variables. | |||
| Characteristic | Career development sum score | p Value | |
| Partnership | No | 1.5 (0–10) | 0.97 |
| Yes | 2 (0–11) | ||
| Partner working as a physician | No | 1 (0–11) | 0.16 |
| Yes | 2 (0–11) | ||
| Family with children | No | 1 (0–11) | 0.09 |
| Yes | 2 (0–11) | ||
| Doing the housework 100% myself | No | 2 (0–11) | 0.09 |
| Yes | 1 (0–10) | ||
| Occupation outside of surgery | No | 2 (0–11) | 0.88 |
| Yes | 2 (0–11) | ||
| Mentor-mentee relationship present | No | 1 (0–11) | 0.09 |
| Yes | 2 (0–11) | ||
| Values are median (range). | |||
The results of the present report show that only slightly more than half of female surgeons and surgical residents in Switzerland have a mentor, and that one-third of the female surgeons do not fulfil a single objective criteria which is considered to be important for an academic career. As would be expected, the sum score of career development was significantly higher when choosing an academic career and also when not intending to become a surgeon with a private practice. A positive influence on career development was found with mentor-mentee relationships or with support in doing the housework. Mentoring significantly enhanced professional advancement with a trend towards increased research productivity. Whether the respondents had children or not, did not have a negative effect on career development.
The prevalence of a mentor-mentee relationship and the small proportion of female mentors in our study is in accordance with other studies [36, 37]. As the possibility of parental leave and a straightforward career are more important for women than for men [3, 38], one would assume that female mentors could be more helpful in giving advices to their mentees compared to their male counterparts. Nevertheless, the relationship was not rated as more helpful and the satisfaction in terms of support in career advancement was not higher with female mentors, which is a controversial topic in the literature [3, 38].
According to Buddeberg et al., participation in a mentoring programme has to be voluntary [39]. Our results are in accordance with this observation as an institutionalised mentoring programme was not associated with additional improvements compared to other mentor-mentee relationships. Nevertheless, the provision of resources in the sense of space for group meetings and financial means should be strongly encouraged, as well as the public notice of mentorship projects [39].
Mentorship has been identified to be an important factor for personal development, career guidance, career choice and career success [40]. It has been found to be a core component to pursue an academic career [2]. Surprisingly, we could not identify a positive influence of mentoring on the plan of an academic career and only a trend towards higher scientific output.
Similarly to previous studies, the main influence of mentoring was found concerning networking and career planning [40, 41].
However, Higgins et al. postulated that not only the quality of a mentor-protégé relationship but also the addition of a supporting network was career relevant [42]. It makes sense that a partner can be helpful in giving support [22]. Still, we could not find an influence just by having a partnership or a partner working in medicine, but we found a positive influence on career success with the presence of support in doing the housework.
It has been shown that a partner who has an understanding for the academic career of his wife, the demands on time and energy that it is taking, and who is willing to let his own wishes take second place, contributes a lot to a successful career advancement of his spouse [22, 43].
Female physicians are more likely to work part-time, especially with the presence of children [44]. It is astonishing that childbearing even leads to a higher objective assessed career development, as it is often linked with interruptions to training [45]. This effect might be caused due to the fact that the women in our study with children were significantly older than those without and thus had probably more time for research. In subjectively assessed career-success ratings, females with children have the lowest values [46]. They report more problems with childcare compared to their male colleagues with slower self-perceived career progress and lower career satisfaction [47]. The objective results regarding this differ in the literature, but positive influences have not yet been found in other studies. Buddeberg et al. did not find a significant influence of having children on career success, whereas others found that women with children were faced with greater obstacles to academic careers and received less institutional support [17, 48]. To cope with time consuming travelling and to generally reduce stress it might be helpful to offer all-embracing child care facilities at work [49].
Beside the institutional career support, a career-oriented professional attitude and personality traits are positively associated with career success [50]. Women are not as interested in research and an academic career as their male colleagues. They are less proactive, have lower professional self-efficacy and are often uncertain as to whether they will be able to balance work and family obligations [34]. Nevertheless, we found that almost one-tenth of participants were aiming for an academic career which is comparable to other studies [17].
Just as important are obstacles of gender stereotypes from superiors [28]. Superiors do not believe that women are as interested in and as capable of an academic career as men [51].
Physicians who aspire to have an academic career have to be successful researchers, in addition to standing out with excellent clinical work [21]. References for successful research are publications and talks at conferences [32-35]. We found that over half of the respondents had not published and one-third had not given any talks. A reason for this might be that women need more encouragement to become researchers [52].
It is necessary to regularly reserve time for research at an early stage of one’s career in order to pursue an academic career successfully [21]. One-sixth of the respondents were engaged in research projects and had a period of research as a principal activity, which is compatible with the one-tenth of women aspiring for an academic career. Nevertheless, there was a lack of awarded third-party funds and scholarships, which reflects the quality of research. Women are less interested in scholarships compared to their male counterparts [53].
Women are known to be more motivated by helping other people than by outside recognition and spend more time with patients than their male colleagues [54]. As a consequence female physicians have lower publication rates and talks at conferences.
On January 1st, 2005, work-hour restrictions for all residency programmes in Switzerland, including a 50-hour working week limitation, became effective [55]. The reduction of time pressure and flexible working hours belong to the most important factors to increase the attractiveness of surgery [29]. It is known that lifestyle considerations are more important for younger generations [56]. More time due to less clinical duties enables an additional pursuit of research [21, 57]. The impact of work-hour restrictions on the interest in a surgical career and an academic pursuit remains unclear as yet.
A limitation of this study was the methodological setting, as a survey based on subjective information. While our low response rate from female surgeons was comparable with that of other surveys among surgeons [58], it still can lead to a non-responder bias and jeopardise the survey’s validity [59].As the current study lacked a matched population of male surgeons, gender differences in surgical academic careers could not be identified. Furthermore we have no information on the evolution in career perceptions, because there was not a prospective cohort.
In conclusion, more than half of the medical school graduates in Switzerland are women but, compared to their male colleagues, only a small proportion show an interest in an academic pursuit. Root causes are the personal attitude and the extent of support by a partner, but the present study also shows the importance of a mentor-mentee relationship. In the early stages of specialty training, the fraction of female residents in an academic career is known to be higher. A supporting network, especially in terms of a mentor, and the absence of obstacles by superiors are crucial, not only so that female physicians interested in an academic career get an opportunity to accomplish their purpose but also so that we do not lack young academics in the near future. An early identification of potential academic candidates and support by providing mentorships and support in family responsibilities would enhance the possibility of combining an academic career with having children. There is considerable potential for improvement as almost half of the respondents did not have a mentor. Further research including a matched population of male surgeons is needed to reveal gender differences in surgical academic careers in Switzerland in detail.
1 Straus SE, Chatur F, Taylor M. Issues in the mentor-mentee relationship in academic medicine: a qualitative study. Acad Med. 2009;84(1):135–9.
2 Sambunjak D, Straus SE, Marusić A. Mentoring in academic medicine: a systematic review. JAMA. 2006;296(9):1103–15.
3 Levinson W, Kaufman K, Clark B, Tolle SW. Mentors and role models for women in academic medicine. West J Med. 1991;154(4):423–6.
4 Wasserstein AG, Quistberg DA, Shea JA. Mentoring at the University of Pennsylvania: Results of a faculty survey. J Gen Intern Med. 2007;22(2):210–4.
5 Applegate WB, Williams ME. Career development in academic medicine. Am J Med. 1990;88(3):263–7.
6 Pearlman SA, Leef KH, Sciscione AC. Factors that affect satisfaction with neonatal-perinatal fellowship training. Am J Perinatol. 2004;21(7):371–5.
7 Wise MR, Shapiro H, Bodley J, Pittini R, McKay D, Willan A, Hannah ME. Factors affecting academic promotion in obstetrics and gynaecology in Canada. J Obstet Gynaecol Can. 2004;26(2):127–36.
8 Levinson DJ, editor. The Seasons of a Man's Life. New York: Alfred A. Knopf, Inc.; 1978.
9 Gonzales AO, Westfall J, Barley GE. Promoting medical student involvement in primary care research. Fam Med. 1998;30(2):113–6.
10 Woessner R, Honold M, Stehle I, Stehr S, Steudel WI. Faculty mentoring programme--ways of reducing anonymity. Med Educ. 1998;32(4):441–3.
11 Buddeberg-Fischer B, Klaghofer R, Abel T, Buddeberg C. Junior physicians’ workplace experiences in clinical fields in German-speaking Switzerland. Swiss Med Wkly. 2005;135(1-2):19–26.
12 Debas HT. Surgery: a noble profession in a changing world. Ann Surg. 2002;236(3):263–9.
13 Federal statistical office. BFS / SHIS, Studierende und Abschlüsse der schweizerischen Hochschulen [homepage on the Internet]; c2011 [cited 2011 Apr 1]. Available from: http://www.bfs.admin.ch/bfs/portal/de/index/themen/15/06/data.html .
14 FMH-Ärztestatistik 2008. Swiss Medical Association (FMH) [homepage on the Internet]; c2011 [cited 2011 Apr 1]. Available from: http://www.fmh.ch/themen/aerztedemographie/aerztestatistik.html.
15 Gjerberg E. Medical women – towards full integration? An analysis of the specialty choices made by two cohorts of Norwegian doctors. Soc Sci Med. 2001;52(3):331–43.
16 Allen I. Women doctors and their careers: what now? BMJ. 2005;331(7516):569–72.
17 Buddeberg-Fischer B, Stamm M, Buddeberg C, Klaghofer R. Career-success scale – a new instrument to assess young physicians' academic career steps. BMC Health Serv Res. 2008;8:120.
18 Bowles AO, Kevorkian CG, Rintala DH. Gender differences regarding career issues and promotion in academic physical medicine and rehabilitation. Am J Phys Med Rehabil. 2007;86(11):918–25.
19 Reichenbach L, Brown H. Gender and academic medicine: Impacts on the health workforce. BMJ. 2004;329(7469):792–5.
20 Tesch BJ, Wood HM, Helwig AL, Nattinger AB. Promotion of women physicians in academic medicine. Glass ceiling or sticky floor? JAMA. 1995;273(13):1022–5.
21 Güller U, Kempski O, Zuber M. The bumpy path to successful academic surgery: a roadmap for the surgical resident. Eur Surg Res. 2009;43(3):253–5.
22 Theorell T. Changing society: changing role of doctors. The stresses must not be allowed to get too great. BMJ. 2000;320(7247):1417–8.
23 Dumelow C, Littlejohns P, Griffiths S. Relation between a career and family life for English hospital consultants: qualitative, semistructured interview study. BMJ. 2000;320(7247):1437–40.
24 Shollen SL, Bland CJ, Finstad DA, Taylor AL. Organizational climate and family life: How these factors affect the status of women faculty at one medical school. Acad Med. 2009;84(1):87–94.
25 Reed V, Buddeberg-Fischer B. Career obstacles for women in medicine: an overview. Med Educ. 2001;35(2):139–47.
26 Gjerberg E. Women doctors in Norway: the challenging balance between career and family life. Soc Sci Med. 2003;57(7):1327–41.
27 Buddeberg-Fischer B, Klaghofer R, Abel T, Buddeberg C. Swiss residents’ speciality choices – impact of gender, personality traits, career motivation and life goals. BMC Health Serv Res. 2006;6:137.
28 Gargiulo DA, Hyman NH, Hebert JC. Women in surgery: do we really understand the deterrents. Arch Surg. 2006;141(4):405–7.
29 Kaderli R, Guller U, Muff B, Stefenelli U, Businger A. Women in Surgery – a Survey in Switzerland. Arch Surg. 2010;145(11):1119–21.
30 Noe RA. An investigation of the determinants of successful assigned mentoring relationships. Personnel Psychology. 1988;41:457–79.
31 Riley S, Wrench D. Mentoring among women lawyers. Journal of Applied Social Psychology. 1985;15:374–86.
32 Carr PL, Ash AS, Friedman RH, Scaramucci A, Barnett RC, Szalacha L, et al. Relation of family responsibilities and gender to the productivity and career satisfaction of medical faculty. Ann Intern Med. 1998;129(7):532–8.
33 Beasley BW, Wright SM. Looking forward to promotion: characteristics of participants in the Prospective Study of Promotion in Academia. J Gen Intern Med. 2003;18(9):705–10.
34 Levinson W, Rubenstein A. Mission critical – integrating clinician-educators into academic medical centers. N Engl J Med. 1999;341(11):840–3.
35 Buddeberg-Fischer B, Leemann R, Klaghofer R. Sociodemographic and career characteristics in female and male faculty members of Swiss medical schools. Swiss Med Wkly. 2003;133(21-22):318–22.
36 Genuardi FJ, Zenni EA. Adolescent medicine faculty development needs. J Adolesc Health. 2001;29(1):46–9.
37 Palepu A, Friedman RH, Barnett RC, Carr PL, Ash AS, Szalacha L, Moskowitz MA. Junior faculty members’ mentoring relationships and their professional development in U.S. medical schools. Acad Med. 1998;73(3):318–23.
38 Park J, Minor S, Taylor RA, Vikis E, Poenaru D. Why are women deterred from general surgery training? Am J Surg. 2005;190(1):141–6.
39 Buddeberg-Fischer B, Vetsch E, Mattanza G. Career support in medicine – experiences with a mentoring program for junior physicians at a university hospital. Psychosoc Med. 2004;1:Doc04.
40 Sciscione AC, Colmorgen GH, D’Alton ME. Factors affecting fellowship satisfaction, thesis completion, and career direction among maternal-fetal medicine fellows. Obstet Gynecol. 1998;91(6):1023–6.
41 Stubbe DE. Preparation for practice: child and adolescent psychiatry graduates’ assessment of training experiences. J Am Acad Child Adolesc Psychiatry. 2002;41(2):131–9.
42 Higgins MC, Kram KE. Reconceptualizing mentoring at work: a developmental network perspective. Academy of Management Review. 2001;26:264–88.
43 Buddeberg-Fischer B, Stamm M, Buddeberg C. Academic career in medicine: requirements and conditions for successful advancement in Switzerland. BMC Health Serv Res. 2009;9:70.
44 Saalwachter AR, Freischlag JA, Sawyer RG, Sanfey HA. Part-time training in general surgery: results of a web-based survey. Arch Surg. 2006;141(10):977–82.
45 Potee RA, Gerber AJ, Ickovics JR. Medicine and motherhood; Medicine and motherhood: shifting trends among female physicians from 1922 to 1999. Acad Med. 1999;74(8):911–9.
46 Buddeberg-Fischer B, Stamm M, Buddeberg C, Bauer G, Häemmig O, Knecht M, Klaghofer R. The impact of gender and parenthood on physicians’ careers – professional and personal situation seven years after graduation. BMC Health Serv Res. 2010;10:40.
47 Limacher MC, Zaher CA, Walsh MN, Wolf WJ, Douglas PS, Schwartz JB, et al. The ACC professional life survey: career decisions of women and men in cardiology. A report of the Committee on Women in Cardiology. American College of Cardiology. J Am Coll Cardiol. 1998;32(3):827–35.
48 Davidson JM, Lambert TW, Goldacre MJ. Career pathways and destinations 18 years on among doctors who qualified in the United Kingdom in 1977: postal questionnaire survey. BMJ. 1998;317(7170):1425–8.
49 Troppmann KM, Palis BE, Goodnight JE Jr, Ho HS, Troppmann C. Women surgeons in the new millennium. Arch Surg. 2009;144(7):635–42.
50 Seibert SE, Crant JM, Kraimer ML. Proactive personality and career success. J Appl Psychol. 1999;84(3):416–27.
51 Bickel J. Women in academic medicine. J Am Med Womens Assoc. 2000;55(1);10–12,19.
52 Schlichting E, Nielsen HB, Fosså SD, Aasland OG. Women’s academic careers in medicine. Tidsskr Nor Laegeforen. 2007;127(16):2109–12.
53 Buckley LM, Sanders K, Shih M, Kallar S, Hampton C. Obstacles to promotion? Values of women faculty about career success and recognition. Committee on the Status of Women and Minorities, Virginia Commonwealth University, Medical College of Virginia Campus. Acad Med. 2000;75(3):283–8.
54 Wright SM, Beasley BW. Motivating factors for academic physicians within departments of medicine. Mayo Clin Proc. 2004;79(9):1145–50.
55 SECO Web site. Application of the labour law to residents working in public hospitals [homepage on the Internet];c2004 [cited 2011 Jun 1]. Available from: http://www.seco.admin.ch/aktuell/00277/01164/01980/index.html?lang=de&msg-id=9333.
56 Henningsen JA. Why the numbers are dropping in general surgery: the answer no one wants to hear-lifestyle! Arch Surg. 2002;137:255–6.
57 Stamp T, Termuhlen P, Miller S, Nolan D, Hutzel P, Gilchrist J, Johnson RM. Before and after resident work hour limitations: an objective assessment of the well-being of surgical residents. Curr Surg. 2005;62(1):117–21.
58 Leece P, Bhandari M, Sprague S, Swiontkowski MF, Schemitsch EH, et al. Internet versus mailed questionnaires: a controlled comparison (2). J Med Internet Res. 2004;6(4):e39.
59 Bhandari M, Devereaux PJ, Swiontkowski MF, Schemitsch EH, Shankardass K, Spraque S, et al. A randomized trial of opinion leader endorsement in a survey of orthopaedic surgeons: effect on primary response rates. Int J Epidemiol. 2003;32(4):634–6.
Authors’ contributions: Study conception and design: Businger, Muff; Acquisition of data: Businger; Analysis and interpretation of data: Kaderli, Businger; Drafting of manuscript: Kaderli, Businger; Critical revision of manuscript: Kaderli, Muff, Stefenelli, Businger; Statistical analysis: Businger and Stefenelli; Administrative, technical and material support: Businger; Study supervision: Businger; Dr. Businger had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding / potential competing interests: This research was funded by the Müller-Möhl Group, Zurich. Role of the Sponsor: The study sponsor had no role in the design and conduct of the study; the collection, management, analysis, and interpretation of the data; or the preparation, review or approval of the manuscript.