Figure 1
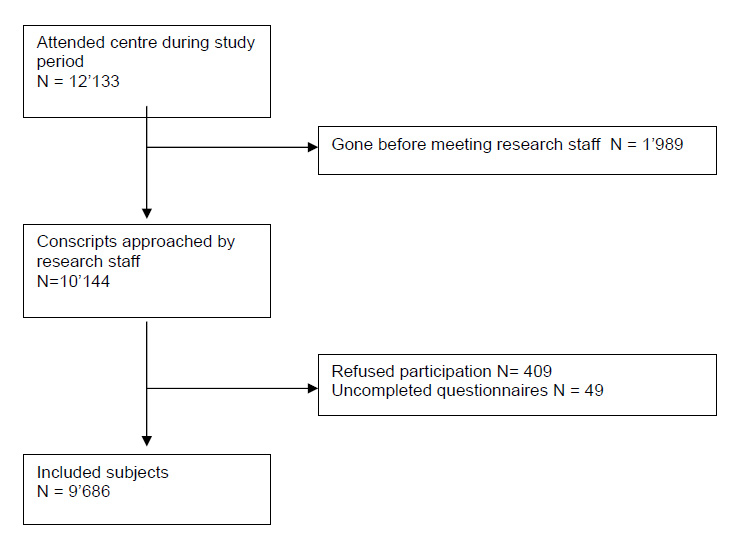
Study flow chart.
DOI: https://doi.org/10.4414/smw.2011.13226
Alcohol is the main substance used and abused by adolescents and young adults [1]. One prevalence study based on data collected from more than 10’000 students in 26 European countries found high rates of alcohol use, drunkenness, and binge drinking among young adults. Alcohol use and misuse was much more widely mentioned than illicit substance use, and any alcohol use in the past month was reported by 82% of the students aged 15–16, compared with 19% reporting use of cannabis within their lifetime, and 7% who had used any other illicit drug at somepoint within their lifetime [1]. Alcohol use is often associated with other health-related behaviours such as tobacco, cannabis and other illicit substance use [2–4]. Many of those who use illicit substances began using alcohol first, and many of them currently still drink [5].
A main public health concern is to more fully understand the influence of alcohol use onset on future risky alcohol use. The relationship between age at first use and later risky alcohol use [6, 7], alcohol abuse and/or dependence (DSM-IV definitions) [8–13] has been investigated often, and most researchers have found that the earlier the onset, the greater the risk to develop alcohol problems.
Few studies have focused on the relationship between early age of first alcohol intoxication and later risky alcohol, tobacco and illicit substance use, even though this is a common pattern. Throughout adolescence, alcohol intoxication becomes progressively more frequent and is associated with numerous risky health behaviours [14]. For example, early age of first alcohol intoxication is associated with a greater risk of unplanned and unprotected sex and unintentional injury [15–17]. There is also an association between hospitalisation for alcohol intoxication and early age of first alcohol intoxication [18].
One study conducted among Southwest California Native Americans showed an association between early age of first alcohol intoxication and later alcohol use disorders (Ehlers and colleagues) [19]. Similarly, among a random sample of the Danish population, Andersen and colleagues showed a strong association between alcohol intoxication at age 15 and excessive consumption by men at age 19 [20].
In countries with mandatory military recruitment procedures, there is an opportunity to evaluate, at a population level, potential associations between age of first intoxication and later alcohol use. The Swiss army recruitment system assesses virtually all males at age 20 to determine service eligibility through a physical, medical and cognitive evaluation of each conscript. Risky single occasion drinking, or binge drinking (BD) (defined as 60 or more g of pure ethanol per occasion), is the most frequent alcohol use pattern in this population [21, 22], and is associated with a greater risk of mortality and morbidity [22–24]. Weekly risky drinking (WRD) occurs less frequently but is associated with a higher risk of alcohol dependence and abuse [25, 26]. It is of interest to describe the association between age of first intoxication and later risky alcohol use patterns, tobacco, cannabis and other illicit substance use in this population. This may help efforts to provide preventive interventions among adolescents and young adults.
This study investigated, in a population-based sample of Swiss men, whether age at first alcohol intoxication is associated with risky alcohol use patterns (BD and WRD) at age 20, and whether age at first alcohol intoxication is associated with tobacco and cannabis use at age 20, and with illicit substance use at somepoint with their lifetime. We hypothesised that early age of first intoxication would be associated with an increased risk of using licit and illicit substances.
A survey of all 20-year-old men attending the Swiss army mandatory recruitment process in Lausanne, Switzerland was conducted between January 2007 and September 2008. These conscripts were from the sector (representing about 21% of the total population) where French is the main language (Bundesamt für Statistik (BFS), 2007). Every young Swiss male is called up for the Swiss army mandatory recruitment. Only young males with an attested severe disablement are excused from the mandatory 2-day army recruitment process. Information could be gained about their education level, professional status and living environment. They were invited to fill out a 5-minute screener containing items on demography, alcohol, tobacco and illicit substance use, and all were informed that the study was not connected to the army in any way and was completely confidential and voluntary. All participants gave written, informed consent, as required by the Ethics Committee for Clinical Research at the Lausanne University Medical School, who approved the study. Data used herein were gathered as part of a larger project encompassing a cohort study and a randomised controlled trial for a brief intervention on risky use or abuse of alcohol. Conscripts were excluded if they left before meeting the research staff, declined to participate or did not fully complete the questionnaire.
The following definition of a standard drink is commonly used in Switzerland: 100 ml of wine; 250 ml of beer; 275 ml of a premixed drink containing spirits; or 25 ml of spirits (containing about 10 g of ethanol each). Weekly risky drinking (WRD) was defined as greater than 21 drinks per week (i.e. 21 x 10 g = 210 g). There are several well-known definitions of risky drinking used in alcohol research. The Clinical Guidelines in Europe and the World Health Organisation suggest 4 or more standard drinks per day (or 280 g/week), and the NIAAA uses 15 or more drinks, or 180–210 g, per week (US Department of Health and Human Services (USDHHS), 2004). A standard drink in the US is 12–14 g, while in Switzerland it is 10 g. The lower definition was chosen for this study because of the young age of the conscripts. The definition of a BD episode used herein was six or more standard drinks (60 g) on a single occasion, and corresponds to both the NIAAA and European definitions. BD was defined as more than one BD episode per month.
The survey questionnaire included questions on the frequency of drinking (“How often do you have a drink containing alcohol?”), on the quantity of alcohol usually drank per drinking day (“How many drinks containing alcohol do you have on a typical day when you are drinking?”), and questions about education level, employment and other demographic characteristics. Each conscript also reported his usual number of BD episodes per month (i.e. “How many times have you had 6 or more standard drinks with alcohol during the same occasion, in a month?”).
Subjects reported current tobacco and cannabis use, as well as use of other illicit substances within their lifetime, such as stimulants (amphetamines or speed), LSD, cocaine, heroin, prescription drugs, hallucinogenic mushrooms, ecstasy and “others”).
Age at first alcohol intoxication (i.e. the first time one became drunk) was determined by asking conscripts if they had even been intoxicated due to alcohol, and if so, at what age it first occurred.
The median age for first intoxication in this sample was 15, so subjects with their first alcohol intoxication before age 15 (n = 3058) were compared with subjects whose first intoxication occurred at 15 or older (or who had never become intoxicated) (n = 6628). Risky alcohol use (WRD and BD) was the primary outcome of interest. Secondary outcomes were current tobacco use, (any current use), cannabis use, (any current use), and illicit substance use within their lifetime.
Analyses were adjusted for the following potential confounding variables: age, employment status (inactive, employed, or in training), highest completed education level (obligatory school versus higher), and household location (urban versus countryside). Confounding variables were selected a priori, based on the prevailing literature and clinical experience.
The association between first intoxication (prior to age 15) with current risky alcohol use (WRD and BD), current tobacco (yes/no) and cannabis use (yes/no) and illicit substance use within their lifetime (yes/no) was assessed using both adjusted and unadjusted logistic regression models, and expressed as odd ratios. The confounding variables listed above were used in the adjusted regressions.
In a second step, and among subjects with a reported intoxication, we evaluated the impact of each additional year of younger occurrence of alcohol intoxication. Zero inflated binomial regressions were used to model the number of drinks per week and the number of BD episodes per month, based on age at first intoxication. The analyses were adjusted for age, living location, education and employment status.
During the study period, 12’133 conscripts attended the recruitment centre, and of these, the research staff saw 10’144 (fig. 1). Of those, 409 refused to participate and 49 did not fully complete the questionnaire. The final sample consisted thus of 9’686 participants.
Figure 1
Study flow chart.
Characteristics of the included subjects are presented in table 1. They were all males with a mean (SD) age of 19.5 (1.2) years. Nearly half (47%) of the participants had completed obligatory school only, more than 70% were currently in training (i.e. professional education, apprenticeship, undergraduate or graduate studies), and about half of them lived in an urban environment. Regarding alcohol use, 89.2% (8,640) reported having been intoxicated from alcohol at least once in the past. The mean (SD) age at first intoxication was 15.0 (1.8) years, and current mean alcohol use (SD) was 9.0 (11.7) drinks per week. The prevalence of WRD and BD was 11.3% and 59.2%, respectively. More than half of the subjects currently used tobacco, 27.5% currently used cannabis, and 19.0% reported use of an illicit substance within their lifetime.
In unadjusted analyses, alcohol intoxication before the age of 15 was significantly associated with risky alcohol use. Compared with subjects who had their first intoxication at age 15 or older (or had no intoxication), subjects who reported having been intoxicated before age 15 were more likely to present current WRD (Odds Ratio [OR]: 3.75, 95% Confidence Interval [CI]: 3.27–4.29) and BD (OR: 3.14, 95% CI: 2.86–3.44). Similarly, alcohol intoxication before age 15 was associated with greater odds of current tobacco use (OR 3.17, 95% CI [2.89–3.47]), current cannabis use (OR 3.26, 95% IC [2.97–3.58]), and illicit substance use at somepoint within their lifetime (OR 4.03, 95% CI [3.62–4.48]). Analyses adjusting for age, education, employment status, and living location yielded comparable results and are presented in table 2.
Among subjects reporting previous intoxication at any age, we conducted additional analyses in order to assess the impact of each additional year of younger occurrence of first intoxication. From age 13–20, each year of younger occurrence of first intoxication was associated with an 18.25% (95%CI: 17.02, 19.45) increase in the number of drinks per week and with a 15.90% (95% CI: 14.55, 17.22) increase in the number of BD episodes per month at the age of 20.
| Table 1: Characteristics of the 9686 included subjects. | |
| Age: mean (SD) | 19.48 (1.18) |
| Education: obligatory school only, % (n) | 47.03 (4543) |
| Occupation: % (n) | |
| Employed | 23.00 (2220) |
| Inactive | 2.82 (272) |
| In training | 74.18 (7160) |
| Living in an urban environment: % (n) | 51.10 (4931) |
| Alcohol use: | |
| Age at first alcohol intoxication: mean (SD) | 15.03 (1.79) |
| Current alcohol use (drinks per week): mean (SD) | 8.99 (11.65) |
| Weekly Risky Drinking (WRD): % (n) | 10.19 (987) |
| Binge drinking (BD): % (n) | 53.39 (5171) |
| Current tobacco use: % (n) | 50.21 (4863) |
| Current cannabis use: % (n) | 27.47 (2658) |
| Illicit substance use at somepoint within their lifetime: % (n) | 18.66 (1781) |
| Education: highest completed education level, obligatory school vs. higher (i.e. professional education, apprenticeship, undergraduate and graduate studies) WRD: weekly risky drinking (>210 g of pure ethanol per week) BD: (more than one occasion per month with ≥60 g of pure ethanol) Tobacco use: any current use Cannabis use: any current use Use of other illegal substances at somepoint within their lifetime (hallucinogenic mushrooms, stimulants (amphetamines, speed), ecstasy, cocaine, LSD, heroine, prescription drug abuse, others) | |
| Table 2: Association between first alcohol intoxication before the age of 15 and risky health behaviours. | |||||
| WRD AOR (95%CI) | BD AOR (95%CI) | Current tobacco use AOR (95%CI) | Current cannabis use AOR (95%CI) | Illicit substance use at somepoint within their lieftime AOR (95%CI) | |
| Age at first alcohol intoxication <15 years old (compared to ≥15 years old or no intoxication) | 3.62 (3.12, 4.20) | 3.10 (2.80, 3.43) | 3.32 (3.00, 3.67) | 3.40 (3.07, 3.77) | 4.20 (3.73–4.72) |
| Confounders | |||||
| Age | 0.98 (0.92, 1.05) | 0.95 (0.91, 0.99) | 1.12 (1.08, 1.17) | 1.10 (1.05, 1.15) | 1.22 (1.16, 1.28) |
| Urban living environment | 0.82 (0.70, 0.95) | 0.74 (0.68, 0.81) | 1.26 (1.15, 1.38) | 1.43 (1.29, 1.58) | 1.31 (1.17, 1.48) |
| Obligatory school only (yes vs. no) | 0.94 (0.80, 1.12) | 1.06 (0.96, 1.17) | 0.70 (0.64, 0.78) | 0.86 (0.77, 0.96) | 0.74 (0.65, 0.85) |
| Occupation (reference group = employed) | |||||
| In training | 0.69 (0.57, 0.82) | 0.87 (0.78, 0.98) | 0.63 (0.56, 0.71) | 0.96 (0.85, 1.10) | 0.67 (0.58, 0.77) |
| Inactive | 0.73 (0.46, 1.15) | 0.84 (0.64, 1.11) | 0.69 (0.52, 0.91) | 1.43 (1.06, 1.92) | 0.96 (0.67, 1.36) |
| AOR: adjusted odds ratio WRD: weekly risky drinking (>210 g of pure ethanol per week) BD: binge drinking (more than one occasion per month with ≥60 g of pure ethanol) Tobacco use: any current use Cannabis use: any current use Use of other illegal substances at somepoint within their lifetime (hallucinogenic mushrooms, stimulants (amphetamines, speed), ecstasy, cocaine, LSD, heroine, prescription drug abuse, others) | |||||
As hypothesised, this study shows an association between an early age of first alcohol intoxication and an increased risk of weekly risky drinking, binge drinking, tobacco, cannabis and other illicit substance use. Subjects who reported first alcohol intoxication before the age of 15 had more than 3 times the odds of risky alcohol and other substance use compared with subjects who reported either a later first alcohol intoxication or who reported never been intoxicated from alcohol, even after adjusting for age, living environment, education and employment status. These strong associations are consistent with the current literature [19, 20]. In addition, we were able to assess the potential impact of each additional year of younger occurrence of alcohol intoxication on drinking at age 20. For each additional year of younger occurrence, we observed a clinically significant increase in drinking at age 20 among subjects who reported at least one episode of alcohol intoxication.
To our knowledge, few studies have focused on the relationship between alcohol intoxication and patterns of risky alcohol use. Ehlers and colleagues conducted a retrospective study in 525 Southwest California Native Americans and reported an association between early age of first intoxication and earlier development of alcohol use disorders [19]. Andersen and colleagues conducted a four-year prospective study of 729 15-year-olds and reported a strong relationship between alcohol intoxication at age 15 and excessive weekly consumption (especially among men) at age 19 (OR: 2.23–3.28) [20]. These two studies differed somewhat in demography, in statistical adjustments within the analyses [19], and in the choice of predictor and outcome variables [19, 20], but showed early-age intoxication to be associated with a greater risk of later risky alcohol use, which is similar to our results. Other research has shown significant associations between an early age of consuming a first alcoholic drink with subsequent heavy drinking [6, 7, 27], or subsequent alcohol abuse or dependence [8–13, 28–30]. The magnitude of the association between the age of first intoxication and weekly risky drinking which the current study found is comparable to other published studies that focused on the link between early age of first intoxication or early alcohol use and later development of risky and/or problem drinking [9, 19, 20, 27].
Nevertheless, other studies have shown that the associations between the age of consuming a first alcoholic drink and alcohol abuse [13] or alcohol dependence [31] were no longer significant when potential confounding factors (i.e., sex, family problems, parental alcoholism or antisocial disorder, and early onset of other substance use) were taken into account. One hypothesis is that a first drink at an early age occurs as a result of a complex behavioural, genetic and environmental interaction, and that early drinking is only part of a broader susceptibility to psychopathology (e.g., disinhibition theory). According to this, early alcohol use would be a marker for an underlying vulnerability to alcohol use disorders, rather than a risk factor [32–36]. We agree that early alcohol use may be a marker of underlying vulnerability, and that the observed associations are not causal in nature. Thus, alcohol intoxication (rather than a single drink) would be expected to have a stronger influence on the development of alcohol addiction but would also introduce more confounding variables, since early intoxication is associated with factors likely to have an impact on the development of alcohol use disorders. An alternative hypothesis for a causal link between early use and later development of alcohol use disorders is that early alcohol use interferes with the course of social and intellectual development, leading to an increased risk of social and psychological diseases, including drug addictions [29]. A recent review stated that an adolescent’s brain, being in a critical phase of development (neuronal maturation, plasticity, synaptic remodelling …), specifically suffers from the adverse effects of alcohol, which probably also influences the specific vulnerability to drug addiction (i.e. mechanisms involved in the neurotoxic, cognitive and neurobehavioural effects of alcohol consumption during adolescence) [37]. The present study design does not allow conclusions to be made in this regard and thus further research (particularly using prospective designs) is needed.
Various studies have shown significant associations between early alcohol use and tobacco, cannabis and substance use [3, 38–42]. McCabe and colleagues [38] reported that early onset of alcohol use was a predictor of concomitant poly-substance use (including alcohol and prescription drugs). Agrawal and colleagues [29] showed, among women, a strong association of onset of alcohol use before age 14 with cannabis use (OR: 13.87) and illicit substance use (OR: 1.44). Wagner and colleagues [29] observed, in 13’105 Mexican students, that early use of either tobacco or alcohol [39] was associated with later use of other drugs, such as cannabis, inhalants, heroin, cocaine and other illicit substances, after adjusting for age, living environment, education and socio-economic level. Our study showed an association between age of first alcohol intoxication with tobacco and cannabis use at age 20, as well as with use of other drugs within their lifetime (including prescription drugs), adding to an accumulation of evidence linking early onset of alcohol use with later substance use.
Nevertheless, some research is not consistent with this evidence. For example, in a study conducted among 12–21 year-olds in the US, Winters and colleagues reported that current cannabis abuse and dependence were not associated with prior onset of drinking [42]. A possible explanation for this is that the use of alcohol and cannabis is often simultaneous [4, 38]. One US research team studied trajectories of substance use among individuals aged 18–26 [43] and observed that the courses of alcohol and cannabis use generated the strongest conjoined trajectory. Similarly, in addition to alcohol use, it has been hypothesised that early use of other substances may be a marker of vulnerability, as mentioned earlier [31, 32, 44, 45].
The present study has limitations. Firstly, because of the cross-sectional design, only associations can be evaluated, and thus our results preclude establishing a causal relationship between early onset of alcohol intoxication and the later development of risky alcohol use patterns. Moreover, age of first intoxication was assessed using a retrospective item making inaccuracy in recall not refutable. Secondly, our sample consisted of men only, although other similar studies have not identified differences between genders [19, 28, 46]. Thirdly, it is possible that the subjects who drink the most will be more likely to report an earlier drinking intoxication, however, our design cannot take into account this source of potential recall bias. Strong efforts were made to minimise potential false reports of substance use, due to hope to avoid military service or in fear of reprisal from the military. To do this, we informed the subjects that where was no relationship or information exchange with the army, and the research staff were clearly identified as not being part of the military personnel. Additionally, our results are consistent with other research, including prospective studies, in which this type of bias is unlikely. Fourthly, the lack of adjustment for duration of exposure to risk may mean that the observed results are over-estimated [28, 46]. It might be expected that the number of years of drinking alcohol (exposure) will be associated with the subsequent development of alcohol use disorders. The duration of exposure is relatively short in the present study, but other researchers using similar exposure times have not considered the lack of adjustment for duration as problematic [12, 28, 47]. Additionally, our study focused on alcohol use, not disorders, at age 20.
Our study has some notable strengths. The sample is large and representative of the entire population of 20-year-old French-speaking Swiss men. We were able to study the association between age at first alcohol intoxication with various risky alcohol use measures, including binge drinking (BD) which is the most prevalent risky behaviour at age 20 among Swiss men.
Our study also has an advantage of being able to provide clear and simple, yet clinically useful information about the associations of early (prior to age 15) first alcohol intoxication with future substance use. Even though this association should not be considered causal, age at first intoxication is information that can easily be obtained during a clinical interview. It can give clinicians important indications of potential occurrences of risky behaviours among their young patients. Clinicians and other health care professionals may use these results to target young populations more likely to develop risky poly-drug use. Since alcohol intoxication may lead to expensive medical care and hospitalisations [18], it can be seen as an opportunity for preventive interventions. Nevertheless, as stated by Zucker and colleagues, it is important for future research to study the trigger elements of first alcohol intoxication and to gain a better understanding of its association with a higher risk of dependence [48].
1 Hibell B, Guttormsson U, Ahlström S, Balakireva O, Bjarnason T, Kokkevi A, et al. The 2007 ESPAD Report: Substance Use Among Students in 35 European Countries. In. The Swedish Council for Information on Alcohol and Other Drugs (editor). Sweden, Stockholm; 2009. pp. 1–408.
2 Brener ND, Collins JL. Co-occurrence of health-risk behaviors among adolescents in the United States. J Adolesc Health. 1998;22(3):209–13.
3 Palmer RH, Young SE, Hopfer CJ, Corley RP, Stallings MC, Crowley TJ, et al. Developmental epidemiology of drug use and abuse in adolescence and young adulthood: Evidence of generalized risk. Drug Alcohol Depend. 2009;102(1–3):78–87.
4 Martin CS, Clifford PR, Clapper RL. Patterns and predictors of simultaneous and concurrent use of alcohol, tobacco, marijuana, and hallucinogens in first-year college students. J Subst Abuse. 1992;4(3):319–26.
5 Kandel D, Faust R. Sequence and stages in patterns of adolescent drug use. Arch Gen Psychiatry. 1975;32(7):923–32.
6 Strunin L, Edwards EM, Godette DC, Heeren T. Country of origin, age of drinking onset, and drinking patterns among Mexican American young adults. Drug Alcohol Depend. 2007;91(2-3):134–40.
7 Hawkins JD, Graham JW, Maguin E, Abbott R, Hill KG, Catalano RF. Exploring the effects of age of alcohol use initiation and psychosocial risk factors on subsequent alcohol misuse. J Stud Alcohol. 1997;58(3):280–90.
8 Pedersen W, Skrondal A. Alcohol consumption debut: predictors and consequences. J Stud Alcohol. 1998;59(1):32–42.
9 Chou SP, Pickering RP. Early onset of drinking as a risk factor for lifetime alcohol-related problems. Br J Addict. 1992;87(8):1199–204.
10 Grant BF, Dawson DA, Stinson FS, Chou SP, Dufour MC, Pickering RP. The 12-month prevalence and trends in DSM-IV alcohol abuse and dependence: United States, 1991–1992 and 2001–2002. Drug Alcohol Depend. 2004;74(3):223–34.
11 Hingson RW, Heeren T, Winter MR. Age at drinking onset and alcohol dependence: age at onset, duration, and severity. Arch Pediatr Adolesc Med. 2006;160(7):739–46.
12 Grant BF, Dawson DA. Age at onset of alcohol use and its association with DSM-IV alcohol abuse and dependence: results from the National Longitudinal Alcohol Epidemiologic Survey. J Subst Abuse. 1997;9:103–10.
13 Grant BF, Stinson FS, Harford T. The 5-year course of alcohol abuse among young adults. J Subst Abuse. 2001;13(3):229–38.
14 Zaborskis A, Sumskas L, Maser M, Pudule I. Trends in drinking habits among adolescents in the Baltic countries over the period of transition: HBSC survey results, 1993–2002. BMC Public Health 2006; 6:67.
15 Hingson R, Heeren T, Winter MR, Wechsler H. Early age of first drunkenness as a factor in college students' unplanned and unprotected sex attributable to drinking. Pediatrics. 2003;111(1):34–41.
16 Hingson R, Heeren T, Zakocs R, Winter M, Wechsler H. Age of first intoxication, heavy drinking, driving after drinking and risk of unintentional injury among U.S. college students. J Stud Alcohol. 2003;64(1):23–31.
17 DuRant RH, Smith JA, Kreiter SR, Krowchuk DP. The relationship between early age of onset of initial substance use and engaging in multiple health risk behaviors among young adolescents. Arch Pediatr Adolesc Med. 1999;153(3):286–91.
18 Wicki M, Gmel G. Alkohol-Intoxikationen Jugendlicher und junger Erwachsener. Ein Update der Sekundäranalyse derDaten Schweizer Hospitäler bis 2005. In. Swiss Institute for the Prevention of Alcohol and Drug Problems (editor). Lausanne, Switzerland; 2008. pp. 1–8.
19 Ehlers CL, Slutske WS, Gilder DA, Lau P, Wilhelmsen KC. Age at first intoxication and alcohol use disorders in Southwest California Indians. Alcohol Clin Exp Res. 2006;30(11):1856–65.
20 Andersen A, Due P, Holstein BE, Iversen L. Tracking drinking behaviour from age 15–19 years. Addiction. 2003;98(11):1505–11.
21 Gmel G, Gaume J, Faouzi M, Kulling JP, Daeppen JB. Who drinks most of the total alcohol in young men – risky single occasion drinking as normative behaviour. Alcohol Alcohol. 2008;43(6):692–7.
22 Rehm J, Taylor B, Room R. Global burden of disease from alcohol, illicit drugs and tobacco. Drug Alcohol Rev. 2006;25(6):503–13.
23 Hingson R, Heeren T, Winter M, Wechsler H. Magnitude of alcohol-related mortality and morbidity among U.S. college students ages 18–24: changes from 1998 to 2001. Annu Rev Public Health. 2005;26:259–79.
24 Perkins HW. Surveying the damage: a review of research on consequences of alcohol misuse in college populations. J Stud Alcohol Suppl. 2002(14):91–100.
25 Reid SC, Ukoumunne OC, Coffey C, Teesson M, Carlin JB, Patton GC. Problem alcohol use in young Australian adults. Aust N Z J Psychiatry. 2007;41(5):436–41.
26 Gmel G, Kuntsche E, Wicki M, Labhart F. Das European School Survey Project on Alcohol and Other Drugs (ESPAD) in der Schweiz: Wichtigste Ergebnisse im Vergleich 2003 und 2007. In. Swiss Institute for the Prevention of Alcohol and Drug Problems (editor). Lausanne; 2009.
27 Pitkanen T, Lyyra AL, Pulkkinen L. Age of onset of drinking and the use of alcohol in adulthood: a follow-up study from age 8–42 for females and males. Addiction. 2005;100(5):652–61.
28 Dawson DA, Goldstein RB, Chou SP, Ruan WJ, Grant BF. Age at first drink and the first incidence of adult-onset DSM-IV alcohol use disorders. Alcohol Clin Exp Res. 2008;32(12):2149–60.
29 DeWit DJ, Adlaf EM, Offord DR, Ogborne AC. Age at first alcohol use: a risk factor for the development of alcohol disorders. Am J Psychiatry. 2000;157(5):745–50.
30 Gruber E, DiClemente RJ, Anderson MM, Lodico M. Early drinking onset and its association with alcohol use and problem behavior in late adolescence. Prev Med. 1996;25(3):293–300.
31 King KM, Chassin L. A prospective study of the effects of age of initiation of alcohol and drug use on young adult substance dependence. J Stud Alcohol Drugs. 2007;68(2):256–65.
32 McGue M, Iacono WG, Legrand LN, Malone S, Elkins I. Origins and consequences of age at first drink. I. Associations with substance-use disorders, disinhibitory behavior and psychopathology, and P3 amplitude. Alcohol Clin Exp Res. 2001;25(8):1156–65.
33 Tarter R, Vanyukov M, Giancola P, Dawes M, Blackson T, Mezzich A, et al. Etiology of early age onset substance use disorder: a maturational perspective. Dev Psychopathol. 1999;11(4):657–83.
34 Iacono WG, Carlson SR, Malone SM, McGue M. P3 event-related potential amplitude and the risk for disinhibitory disorders in adolescent boys. Arch Gen Psychiatry. 2002;59(8):750–7.
35 Prescott CA, Kendler KS. Age at first drink and risk for alcoholism: a noncausal association. Alcohol Clin Exp Res. 1999;23(1):101–7.
36 Heath AC, Martin NG. Teenage alcohol use in the Australian twin register: genetic and social determinants of starting to drink. Alcohol Clin Exp Res. 1988;12(6):735–41.
37 Guerri C, Pascual M. Mechanisms involved in the neurotoxic, cognitive, and neurobehavioral effects of alcohol consumption during adolescence. Alcohol. 2010;44(1):15–26.
38 McCabe SE, Cranford JA, Morales M, Young A. Simultaneous and concurrent polydrug use of alcohol and prescription drugs: prevalence, correlates, and consequences. J Stud Alcohol. 2006;67(4):529–37.
39 Wagner FA, Velasco-Mondragon HE, Herrera-Vazquez M, Borges G, Lazcano-Ponce E. Early alcohol or tobacco onset and transition to other drug use among students in the state of Morelos, Mexico. Drug Alcohol Depend. 2005;77(1):93–6.
40 Agrawal A, Grant JD, Waldron M, Duncan AE, Scherrer JF, Lynskey MT, et al. Risk for initiation of substance use as a function of age of onset of cigarette, alcohol and cannabis use: findings in a Midwestern female twin cohort. Prev Med. 2006;43(2):125–8.
41 Takakura M, Wake N. Association of age at onset of cigarette and alcohol use with subsequent smoking and drinking patterns among Japanese high school students. J Sch Health. 2003;73(6):226–31.
42 Winters KC, Lee CY. Likelihood of developing an alcohol and cannabis use disorder during youth: association with recent use and age. Drug Alcohol Depend. 2008;92(1-3):239–47.
43 Jackson KM, Sher KJ, Schulenberg JE. Conjoint developmental trajectories of young adult substance use. Alcohol Clin Exp Res. 2008;32(5):723–37.
44 Kendler KS, Schmitt E, Aggen SH, Prescott CA. Genetic and environmental influences on alcohol, caffeine, cannabis, and nicotine use from early adolescence to middle adulthood. Arch Gen Psychiatry. 2008;65(6):674–82.
45 Kendler KS, Myers J, Prescott CA. Specificity of genetic and environmental risk factors for symptoms of cannabis, cocaine, alcohol, caffeine, and nicotine dependence. Arch Gen Psychiatry. 2007;64(11):1313–20.
46 Pitkanen T, Kokko K, Lyyra AL, Pulkkinen L. A developmental approach to alcohol drinking behaviour in adulthood: a follow-up study from age 8 to age 42. Addiction. 2008;103(Suppl 1):48–68.
47 Richter M, Leppin A, Nic GS. The relationship between parental socio-economic status and episodes of drunkenness among adolescents: findings from a cross-national survey. BMC Public Health. 2006;6:289.
48 Zucker RA, Donovan JE, Masten AS, Mattson ME, Moss HB. Early developmental processes and the continuity of risk for underage drinking and problem drinking. Pediatrics. 2008;121(Suppl 4):S252–S272.
Funding / potential competing interests: The present study was funded by the Swiss Foundation of Alcohol Research