Figure 1
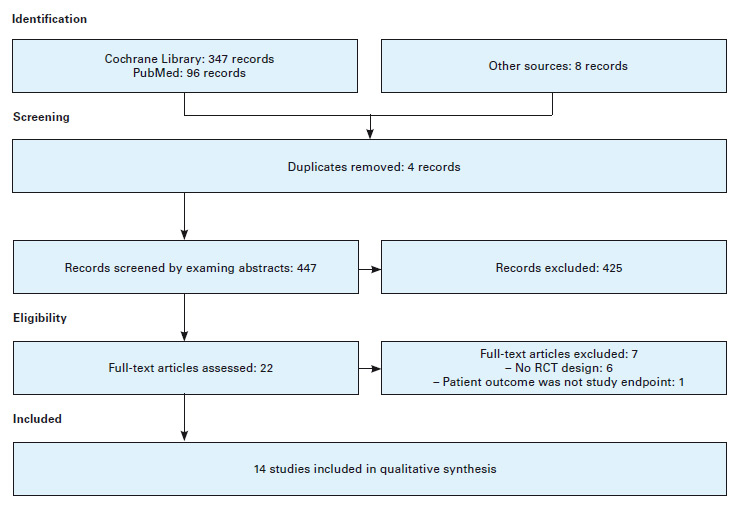
Flow diagram on phases of review process (according to PRISMA statement [13]).
DOI: https://doi.org/10.4414/smw.2010.13062
An increasing volume of literature reports that deficiencies in collaboration and communication between healthcare professionals have a negative impact on the provision of healthcare and on patient outcomes [1–3]. The consequences reach far beyond stress and frustration levels experienced by professionals; they can result in adverse events such as medication errors and failure to rescue [4–7]. The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) is a voluntary organisation that monitors critical incidents and sentinel events in healthcare settings in the USA, which have been defined as “unexpected occurrences involving death or serious physical or psychological injury, or the risk of thereof” [8]. In 2003, JCAHO reported that communication failures among team members are a contributory factor in 60% of sentinel events [9]. The factor most influential in reducing these events and their potentially negative effects on clinical outcomes is improvement of relationships among clinicians [3]. Policymakers, managers and clinicians therefore have a growing interest in intervening in these relationships through two major approaches: 1) quality and safety improvements by systematically analysing care processes, and 2) interprofessional education and interventions to foster collaboration [10]. In particular, new models of care emphasising the need for close interprofessional collaboration and a focus on the use of technology to provide continuous and coordinative care to the aging and chronically ill population in Western countries are often requested in this context [11, 12]. These approaches are fundamental to delivery of safe quality care. To establish new models of care delivery, policymakers, managers, and clinicians need to know how effective interventions on interprofessional collaboration are. This article sets out to provide an overview of the evidence base for interprofessional collaboration and new models of care in relation to patient outcomes. It is not designed as a formal systematic literature review as recommended by PRISMA Group or Cochrane Library [13].
To examine the evidence base for the relationship between interprofessional collaboration and patient outcomes, two of the authors searched the literature independently using the following definition to retrieve salient articles: “Interprofessional collaboration exists when two or more members of different healthcare professions work together jointly to solve problems or provide services [10]. Furthermore, effective collaboration requires shared power and authority, based on knowledge and expertise and an interaction between subjects with trust, mutual respect and joint contributions to a common goal [14].” Several terms are regularly used to describe working together; these include “teamwork” and “collaboration”, and highlight the inconsistencies in defining a complex phenomenon [14]. Moreover, terms such as “multidisciplinary”, “interdisciplinary”, “interprofessional” and “multiprofessional” are often used interchangeably in the literature and their definition depends on people’s attitudes and points of view [15]. Accordingly, we used most of those terms in different combinations to describe collaborations between healthcare professionals. A set of exclusion and inclusion criteria was used to identify relevant articles for the review process. Papers with a clinical focus on care management between two or more healthcare professions, but comprising doctors and nurses, and on patient outcomes were included. In addition, it was important for us to include only articles describing interventions with inherent collaboration of healthcare professionals. Exclusion criteria were publications not relevant to the topic, those dated prior to 1998, and non-research articles.
Figure 1
Flow diagram on phases of review process (according to PRISMA statement [13]).
The initial search included two bibliographic databases (PubMed, CINAHL) with the following key words and Boolean operators (OR, AND) being used as appropriate: “multi-/interdisciplinary collaboration”, “medicine and nursing”, “physicians and nurses” and “new models of care medicine/nursing”. A preliminary reading of the abstracts showed that the articles used a broad range of research designs, with few randomised controlled trials. For that reason a second search was conducted in PubMed and Cochrane Library. In this search, the terms “interdisciplinary collaboration”, “interdisciplinary health team”, “physicians and nurses”, “interprofessional collaboration” and “cooperative behaviour” were used together with the following limits: published within the last ten years, clinical trial, meta-analysis, randomised controlled trial (RCT), review, and restricted to English and German articles. Out of a total of 451 articles, 22 suitable publications meeting the above-mentioned criteria were selected on the basis of the abstract. Randomised controlled trial was added as a selection criterion, since all Cochrane reviews regarding collaboration complained of the lack of RCTs. Two reviewers independently read the complete articles and selected fourteen studies for the final sample, again applying the inclusion criteria specified above. Disagreements on eligibility were resolved by consulting a third reviewer; a majority needed to agree on the inclusion of an article (fig. 1). A data-driven thematic analysis was used to identify prominent themes, and findings of the selected studies were summarised and structured accordingly under thematic headings [16].
All of the fourteen RCTs were conducted in Western countries (table 1); nine from the USA [17–26], three from Europe [27–29], and one each from Australia and Canada [30, 31]. The study samples included between 50 and 500 patients per group. Randomisation referred either to patients or to interventions of primary care physicians. Thus, separation of intervention and control groups sought to prevent contamination of treatment between groups. One study from England included an additional nested qualitative component within the trial, namely patient and practitioner interviews [28]. Eight studies applied a repeated measurement to measure the impact of the intervention over a longer time frame.
Nine RCTs tested collaborative care management models against usual care within the elderly population; seven studies focused on chronic diseases such as heart failure, multimorbidity and Alzheimer’s disease. A single study investigated a collaborative model for paediatric asthma [22]. All but two studies implemented an intervention in outpatient care. Nikolaus and colleagues [27] studied the effect of a comprehensive geriatric assessment and post-discharge home intervention for patients with acute illnesses in a geriatric hospital in Germany. Naglie and colleagues [31] were interested in the outcomes of postoperative interprofessional care management for patients with hip fracture at a university-affiliated acute care hospital in Canada.
The major components of the interventions, based on interprofessional collaboration, included new models of care with bio-psycho-social assessment, development of an individual evidence-based treatment plan, coordination of care, monitoring of health status, coaching patients in chronic disease self-management and promotion of community-based services. Depending on the scope of the intervention, the duration of the programmes included in this review varied between a few days (e.g., a two-visit educational intervention at an outpatient clinic for children with asthma [22]) and two to three years of implementation (e.g., introduction of a system for collaborative primary care for elderly people aged 65 or over [18, 25, 26] or for patients with bipolar disorder [23, 24]).
The most common outcome measures included mortality, clinical, functional and social outcomes, and utilisation of medical services. A majority of studies (n = 9) also involved patient-reported outcomes such as quality of life, activities of daily livingand satisfaction with care.
Five studies reported no difference in mortality between the intervention and usual care groups [17, 21, 25, 27, 31] whereas Schraeder and colleagues [18] reported a 49% reduction in all-cause mortality in the treatment group during the second year (odds ratio: 0.51, 95% CI: 0.29–0.91, p= 0.02). Moreover, Inglis and colleagues [30] observed median survival in patients with chronic heart failure almost twice that of the control group (40 versus 22 months respectively, p <0.001) and fewer deaths overall (adjusted relative risk: 0.74, 95% CI: 0.53–0.80, p <0.001) after up to ten years’ follow-up. In five studies an improvement in physical, emotional or social functioning was demonstrated in the intervention group [19, 24, 27–29], though four studies showed no differences between groups [17, 21, 25, 31]. Similarly mixed results were reported regarding utilisation of medical services. Again, five studies showed a significant reduction in medical service use in the intervention group compared to the control group [17, 20, 22, 27, 30], and two studies reported mixed results. Counsell and colleagues [25] observed that following the intervention there was a significant reduction in emergency department visits without hospitalisation in their low-income elderly population, but no group differences for hospital admission rates. Bauer and colleagues [24] reported a trend towards lower hospitalisation rates for any reason among psychiatric patients in the intervention group during the second year of the study, and a significant reduction in the third year (34 % versus 48%, respectively, p = 0.02). However, two American studies reported no differences regarding hospitalisation rates or length of hospital stay between groups [18, 21].
With regard to patient-reported outcomes, the geriatric intervention group in a German study [27] showed a significantly higher score of self-perceived health and life satisfaction than the control group (p = 0.04). In addition, chronically ill seniors in another American study [17] reported an increase in social activities compared with a decrease in the control group (p = 0.04). Two studies reported no group differences in activities of daily living [21, 25], whereas Melis and colleagues [29] showed a significant improvement in functional abilities during the first six months; after this time, however, the effects were no longer significant. Furthermore, four studies showed that participants who experienced collaborative care management models were significantly more satisfied with their care than usual-care recipients [20, 24–26].
| Table 1Abbreviations: ADL= Activities of daily living/ED = emergency department/ y = years of age/ TIA = transient ischaemic attack/CI = confidence interval | |||||
| Authors, date, country | Setting, patient population | Intervention/model of care, providers | Outcomes measures | Participants | Selected results |
| Nikolaus et al., 1999Germany | In- , outpatient care, patients (>65 y) with acute diseases | Geriatric care management and postdischarge intervention over a mean period of 7.6 days; nurse, physio-, occupational therapist, social worker, primary care physician | Survival, functional status, hospital readmission, nursing home placement, direct costs | 181 assessment and intervention,179 assessment only,185 usual care | 12-month follow-up: intervention group had better functional abilities (p = 0.03), higher score of self-perceived health and life satisfaction (p = 0.04). Mortality in all groups was similar, but intervention group had a reduction in length of hospital stay, rate of immediate nursing home placement (p <0.05) and costs. |
| Sommers et al., 2000California, USA | Primary care, elderly patients with chronic illnesses | Collaborative practice model over 18 months; geriatric nurse, social worker, primary care physician | Utilisation of medical services and changes in patient self-rated physical, emotional and social functioning | 280 intervention,263 usual care | First year: groups did not differ in the study endpoints.Second year: hospitalisation rate (p = 0.03), readmission rate (p = 0.03) and mean office visits (p = 0.003) increased significantly in the control compared to intervention group. Mortality did not differ between the two groups over both years. |
| Schraeder et al., 2001Illinois, USA | Primary care,patients (>65 y) with risk factors | Collaborative model of primary care for 24 months;nurse, case assistent, primary care physician | Mortality and hospital use | 530 intervention, 411 usual care | 12- and 24-month follow-up: intervention group had a 49% reduction in mortality during second year of study (p = 0.02). No difference between groups in hospitalisation rate and length of hospital stay, although the treatment group was sicker at baseline. |
| Allen et al., 2002Ohio, USA | Primary care,patients after stroke or TIA | Postdischarge care model for stroke and TIA over 3 months; advanced practice nurse, interdisciplinary team, primary care physician | Neuromotor function, severe complications, quality of life, risk management, strokeknowledge | 47 intervention,46 usual care | At 3-months postdischarge: Care management model significantly improved the profile of health and prevention (p <0.0001) in the intervention group. Moreover the effect size for each domain was positive with the highest for stroke knowledge (0.98) and the smallest for neuromotor function (0.10). |
| Naglie et al., 2002Ontario, Canada | Inpatient care, patients (>70 y) with hip fracture who underwent surgical repair | Postop. interdisciplinary care over a mean period of 29.2 days; geriatrician, clinical nurse specialist, physio-, occupational therapist, social worker | Proportion of patients alive, decline in ambulation or transfers, change in place of residence | 141 intervention,138 usual care | Analysis showed no significant difference between intervention and control groups at 3- and 6-month follow-up. A subgroup analysis suggested a benefit for patients with mild to moderate cognitive impairment. |
| Krein et al., 2004Michigan, USA | Primary care,patients with poorly controlled type 2 diabetes | Collaborative case management over 18 months; nurse practitioner, primary care physician | Glycaemic control, intermediate cardio-vascular outcomes, satisfaction with care, resource utilisation | 110 intervention,106 usual care | No differences between groups regarding HbA1c exit levels, cholesterol levels or blood pressure control. But intervention patients were significantly more satisfied with their care (p = 0.04) and received less care outside the Veterans Affairs (p = 0.007). |
| Callahan et al., 2006Indianapolis USA | Primary care,patients with Alzheimer disease | Collaborative care model over 1 year; advanced practice nurse, primary care physician, geriatrician, psychiatrist, psychologist | Neuropsychiatric inventory, depression, cognition, ADL, resource use | 84 intervention,69 augmented usual care | 6-, 12- and 18-month follow-up: intervention group had significantly fewer behavioural and psychological symptoms of dementia at 12 and 18 months (p = 0.01). No group difference in depression, cognition, ADL, hospitalisation rates, nursing home placement or death. |
| Inglis et al., 2006South Australia | Primary care,patients with chronic heart failure | Chronic heart failure programme over 6 months;(cardiac) nurse, pharmacist, primary care physician, cardiologist | All-cause mortality,event-free survival, recurrent hospital stay, cost per life-year gained | 149 intervention,148 usual care | 10-year follow-up: Median survival of intervention group was almost twice that of control group (p <0.001) with lower death rate (p <0.001), and associated with longer event-free survival (p <0.01). Rates of readmissions and related hospital stay were also significantly lower in the intervention group. |
| Walders et al., 2006Colorado, USA | Outpatient clinic,children (4–12 Y) with asthma | Interdisciplinary intervention for paediatric asthma during 2 visits to medical centre;nurse, social worker, psychologist, pulmonologist | Differences in asthma symptom reports, health care utilisation, quality of life | 89 intervention,86 usual care | 12-month follow-up: both groups showed reductions in asthma symptoms and improvements in quality of life without differences between groups. But intervention group had fewer health care utilisation than control group (p = 0.05). |
| Bauer et al., 2006 Part 1 and 2, Rhode Island, USA | Mental health outpatient clinic, patients with bipolar disorder | Collaborative chronic care over 3 years;nurse care coordinator, psychiatrist | Clinical and functional outcome, quality of life, additional clinical service use | 157 intervention,157 usual care | Follow-up every 8 weeks: intervention group had significantly reduced weeks in affective episode, primarily mania and improved social role functioning. No significant reduction in mean manic and depressive symptoms. Follow-up every 24 weeks: improvement in mental quality of life (p = 0.01) and treatment satisfaction (p <0.001) in the intervention group. |
| Chew-Graham et al., 2007England | Primary care,patients (>60 y) with depression | Collaborative care model over 12 weeks;psychiatric nurse, primary care professionals, psychiatrist | Recovery from depression, acceptability of intervention (nested qualitative study) | 53 intervention,52 usual care | 16-week follow-up: intervention group had fewer major depressive disorders than control group (p = 0.036). Adjusted odds ratio for depression was 0.32 (95% CI: 0.11–0.93). Interviews with patients and practitioners demonstrated the effectiveness and acceptability of the intervention. |
| Counsell et al., 2007Indianapolis USA | Primary care,patients (>65 y) with low-income | Geriatric care management model over 2 years;nurse practitioner, social worker, primary care physician, geriatric team | Quality of medical care, ADL, quality of life, ED visits without hospitalisation, hospitalisations | 474 intervention,477 usual care | 6-, 12-, 18- and 24-month follow-up: intervention group had significant improvement in quality of care and reduced ED utilisation rate (p = 0.03). No group differences for hospital admission rates, ADL or death. |
| Melis et al., 2008Netherlands | Primary care,patients (>70 y) with problems in cognition, ADL | Problem-based, geriatric intervention over 3 months;geriatric nurse, primary care physician, geriatrician | Functional abilities in ADL, mental well-being | 85 intervention,66 usual care | 3- and 6-month follow-up: significant improvement in functional abilities and mental well-being in the intervention group. After 6 months, effects increased for well-being but functional abilities were no longer significant. |
| Boult et al., 2008Maryland, USA | Primary care,patients (>65 y) with multi-morbidity | Guided care model over 2 years;nurse, primary care physician, caregiver at home | Patients’ perception of their quality of health care, professionals’ satisfaction with care | 408 intervention,359 usual care | 6- and 12-month follow-up: intervention group was about twice as likely to rate their overall care as “high quality” (p = 0.006). Primary care physician were more satisfied with their interactions with patients and their families (p <0.05) and nurses expressed a consistently high job satisfaction. |
Interprofessional collaboration is a common strategy to achieve desired quality outcomes in an effective and efficient manner in a complex array of health services [32]. Nowadays, improved interprofessional collaboration is essential to facilitate information flow and the coordination and provision of healthcare within an increasing diversity of disciplines where one health professional can no longer meet all patient needs [33–35].
This literature review provides an overview of the evidence base of interprofessional collaboration and its relationship to patient outcomes. Our main finding was that the vast majority of the eligible publications indicate at least one improved outcome following interventions based on interprofessional collaboration.
Most of the studies included introduced new models of care with promising approaches to service delivery, yet some have methodological shortcomings such as sample sizes inadequate to reach satisfactory power levels or longer time frames over which outcome is measured, resulting in patient withdrawal and missing data. Nevertheless, the studies’ longer time frames were probably beneficial in making it possible to introduce complex interventions properly and judge the sustainability of programme effects. An additional weakness of several studies was that some outcome measures were collected by nurses who were included in the intervention and not blinded to participants’ status, a factor which may have had an impact on the results. More importantly, most of the models tested were multifaceted, rendering separation of the impact of collaboration from other parts of the intervention impossible. The research instruments applied in the RCTs included mainly measured patient-related outcomes such as the Barthel Index, the Short Mental Status Questionnaire, and the National Institutes of Health Stroke Scale. Other databases such as death registries and medical record systems were also used. Collaboration was not a study endpoint and hence questionnaires specific to this issue were not used.
Overall the relationships between teamwork and patient outcomes seem to be difficult to investigate with RCTs, since we can only compare a facilitated, more structured collaboration with a routine form of collaboration. In a previous Cochrane review on interventions to promote collaboration between nurses and doctors, the authors concluded that rigorous evaluations are difficult to conduct because the interventions are complex and the intermediate processes are difficult to assess [36]. This review only included two out of 31 studies which tested interventions in academic hospital settings with acceptable methodological quality [37, 38]. The two trials could not demonstrate effects on mortality and only moderate gains in healthcare processes. A few years later a second systematic review on the effects of interventions on interprofessional collaboration and education [10] yielded fourteen studies in the area of collaboration. Of the studies included five reported no difference in outcomes and nine showed improved results related to their interventions, suggesting a positive impact of interprofessional collaboration interventions on healthcare pro-cesses and outcomes [10].
Although RCTs are the gold standard in establishing a sound evidence base in quantitative research, results from other studies may be crucial in adequately interpreting this evidence, formulating research questions and designing future studies. RCTs may establish causal relationships but do not identify causal processes, which are also important in health services research. Hence investigations into the English health services increasingly use qualitative research methods alongside RCTs in order to gain a more comprehensive understanding of the impact of health service delivery and organisation [39]. Complex practice settings often require more diverse methodology.
For example, observational studies of the processes and performances of patient care teams show that teamwork is an important factor in the causation and prevention of adverse events [7]. A very recent publication on the impact of surgical team behaviours on patient outcomes reported increased odds on major complications or death when the team less frequently shared information during intraoperative phases and handoff phases [40]. Moreover, all measures of poor teamwork across all intraoperative phases were significantly associated with deteriorated patient outcome after adjusting for the American Society of Anaesthesiologists (ASA) score. Therefore, restriction to RCTs alone is a limitation of our review.
Barriers to good interprofessional relationships described in the literature include time pressure, lack of explicit descriptions or of understanding of each other’s roles and tasks, poor organisational support, absence of clear leadership, different traditions and professional values, different aims and priorities, and vertical management structures with discriminatory power structures [35, 41–43]. To identify factors that enable nurse and physician collaboration, an American study investigated the literature and additionally interviewed 141 physicians, managers and staff nurses from 44 clinical units in five hospitals [44]. Structural enablers included joint nurse/physician practice committees, integrated patient records, joint practice record review, and the use of protocols or critical pathways in the care of specific patient groups. With regard to interpersonal relationships and interactions, they mentioned trust, respect, shared leadership, recognition of unique contribution, collegiality, and open communication as en-abling factors [44].
In summary, although the studies included reported mixed results, all but one study identified at least one positive and statistically significant effect of the collaborative care models tested. Nevertheless, additional research is needed in this field involving different patient populations and including inpatient care. Two interesting studies are currently under way. One is a cluster randomised controlled trial in five tertiary-care hospitals in Toronto to investigate an intervention with the aim of improving collaborative communication between healthcare professionals and patient-centred care [45]. The second study is a cluster randomised controlled trial in primary care in Australia which seeks to determine the impact of nurse and general practitioner partnership on the quality of care and patient outcomes for patients with chronic obstructive pulmonary disease [46].
Up to now the evidence base of interprofessional collaboration shows promising results in relation to patient outcomes, thus justifying further implementation of new models of service delivery in clinical practice which supports collaboration between professionals.
1 Fagin CM. Collaboration between nurses and physicians: no longer a choice. Acad Med. 1992;67(5):295–303.
2 Makary MA, Sexton JB, Freischlag JA, Holzmueller CG, Millman EA, Rowen L, et al. Operating room teamwork among physicians and nurses: teamwork in the eye of the beholder. J Am Coll Surg. 2006;202(5):746–52.
3 Rosenstein AH, O’Daniel M. Disruptive behavior and clinical outcomes: perceptions of nurses and physicians. Am J Nurs. 2005;105(1):54–64.
4 Kohn LT, Corrigan JM, Donaldson MS, editors. To err is human: Building a safer health system, 5th ed. Washington DC: Institute of Medicine, National Academy Press; 2006.
5 Rosenstein AH, O’Daniel M. Impact and implications of disruptive behavior in the perioperative arena. J Am Coll Surg. 2006;203(1):96–105.
6 Manojlovich M, DeCicco B. Healthy work environments, nurse-physician communication, and patients’ outcomes. Am J Crit Care. 2007;16(6):536–43.
7 Manser T. Teamwork and patient safety in dynamic domains of healthcare: a review of the literature. Acta Anaesthesiol Scand. 2009;53(2):143–51.
8 Joint Commission on the Accreditation of Healthcare Organizations. Joint Commission Perspectives 1997 [cited 2008 Sep 18]. Available from: http://www.JointCommission.org .
9 Doran D. Teamwork – Nursing and the Multidisciplinary Team. In: L McGillis Hall, editor, Quality Work Environments for Nurse and Patient Safety. Sudbury, MA: Jones and Bartlett Publishers; 2005; p. 39–66.
10 Zwarenstein M, Reeves S. Knowledge translation and interprofessional collaboration: Where the rubber of evidence-based care hits the road of teamwork. J Contin Educ Health Prof. 2006;26(1):46–54.
11 Giger M, De Geest S. Neue Versorgungsmodelle und Kompetenzen sind gefragt. Schweizerische Ärztezeitung. 2008;89(43):1839–43.
12 De Geest S, Moons P, Callens B, Gut C, Lindpaintner L, Spirig R. Introducing Advanced Practice Nurses / Nurse Practitioners in health care systems: a framework for reflection and analysis. Swiss Med Wkly. 2008;138(43-44):621–8.
13 Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. Bmj. 2009;339:b2700.
14 Henneman EA, Lee JL, Cohen JI. Collaboration: a concept analysis. J Adv Nurs. 1995;21(1):103–9.
15 Gillioz S. Theorie und Praxis der Interdisziplinarität. Journal SRK 1997;3:3–11.
16 Dixon-Woods M, Agarwal S, Jones D, Young B, Sutton A. Synthesising qualitative and quantitative evidence: a review of possible methods. J Health Serv Res Policy. 2005;10(1):45–53.
17 Sommers LS, Marton KI, Barbaccia JC, Randolph J. Physician, nurse, and social worker collaboration in primary care for chronically ill seniors. Arch Intern Med. 2000;160(12):1825–33.
18 Schraeder C, Shelton P, Sager M. The effects of a collaborative model of primary care on the mortality and hospital use of community-dwelling older adults. J Gerontol A Biol Sci Med Sci. 2001;56(2):M106–12.
19 Allen KR, Hazelett S, Jarjoura D, Wickstrom GC, Hua K, Weinhardt J, et al. Effectiveness of a postdischarge care management model for stroke and transient ischemic attack: a randomized trial. J Stroke Cerebrovasc Dis. 2002;11(2):88–98.
20 Krein SL, Klamerus ML, Vijan S, Lee JL, Fitzgerald JT, Pawlow A, et al. Case management for patients with poorly controlled diabetes: a randomized trial. Am J Med. 2004;116(11):732–9.
21 Callahan CM, Boustani MA, Unverzagt FW, Austrom MG, Damush TM, Perkins AJ, et al. Effectiveness of collaborative care for older adults with Alzheimer disease in primary care: a randomized controlled trial. JAMA. 2006;295(18):2148–57.
22 Walders N, Kercsmar C, Schluchter M, Redline S, Kirchner HL, Drotar D. An interdisciplinary intervention for undertreated pediatric asthma. Chest. 2006;129(2):292–9.
23 Bauer MS, McBride L, Williford WO, Glick H, Kinosian B, Altshuler L, et al. Collaborative care for bipolar disorder: part I. Intervention and implementation in a randomized effectiveness trial. Psychiatr Serv. 2006;57(7):927–36.
24 Bauer MS, McBride L, Williford WO, Glick H, Kinosian B, Altshuler L, et al. Collaborative care for bipolar disorder: Part II. Impact on clinical outcome, function, and costs. Psychiatr Serv. 2006;57(7):937–45.
25 Counsell SR, Callahan CM, Clark DO, Tu W, Buttar AB, Stump TE, et al. Geriatric care management for low-income seniors: a randomized controlled trial. JAMA. 2007;298(22):2623–33.
26 Boult C, Reider L, Frey K, Leff B, Boyd CM, Wolff JL, et al. Early effects of “Guided Care” on the quality of health care for multimorbid older persons: a cluster-randomized controlled trial. J Gerontol A Biol Sci Med Sci. 2008;63(3):321–7.
27 Nikolaus T, Specht-Leible N, Bach M, Oster P, Schlierf G. A randomized trial of comprehensive geriatric assessment and home intervention in the care of hospitalized patients. Age Ageing. 1999;28(6):543–50.
28 Chew-Graham CA, Lovell K, Roberts C, Baldwin R, Morley M, Burns A, et al. A randomised controlled trial to test the feasibility of a collaborative care model for the management of depression in older people. Br J Gen Pract. 2007;57(538):364–70.
29 Melis RJ, van Eijken MI, Teerenstra S, van Achterberg T, Parker SG, Borm GF, et al. A randomized study of a multidisciplinary program to intervene on geriatric syndromes in vulnerable older people who live at home (Dutch EASYcare Study). J Gerontol A Biol Sci Med Sci. 2008;63(3):283–90.
30 Inglis SC, Pearson S, Treen S, Gallasch T, Horowitz JD, Stewart S. Extending the horizon in chronic heart failure: effects of multidisciplinary, home-based intervention relative to usual care. Circulation. 2006;114(23):2466–73.
31 Naglie G, Tansey C, Kirkland JL, Ogilvie-Harris DJ, Detsky AS, Etchells E, et al. Interdisciplinary inpatient care for elderly people with hip fracture: a randomized controlled trial. Cmaj. 2002;167(1):25–32.
32 Kurtin SE. Multidisciplinary Clinical Service Teams. In: ML Parsons; CL Murdaugh; TF Purdon et al., editors, Strategies for improving Patient Care: Guide to Clinical Resource Management. Gaithersburg, MD: Aspen Publishers; 1997; p. 66–87.
33 Yeager S. Interdisciplinary collaboration: the heart and soul of health care. Crit Care Nurs Clin North Am. 2005;17(2):143–8, x.
34 McCallin A. Interdisciplinary practice – a matter of teamwork: an integrated literature review. J Clin Nurs. 2001;10(4):419–28.
35 Xyrichis A, Lowton K. What fosters or prevents interprofessional teamworking in primary and community care? A literature review. Int J Nurs Stud. 2008;45(1):140–53.
36 Zwarenstein M, Bryant W. Interventions to promote collaboration between nurses and doctors. Cochrane Database Syst Rev. 2000(2):CD000072.
37 Curley C, McEachern JE, Speroff T. A firm trial of interdisciplinary rounds on the inpatient medical wards: an intervention designed using continuous quality improvement. Med Care. 1998;36(8 Suppl):AS4–12.
38 Jitapunkul S, Nuchprayoon C, Aksaranugraha S, Chaiwanichsiri D, Leenawat B, Kotepong W, et al. A controlled clinical trial of multidisciplinary team approach in the general medical wards of Chulalongkorn Hospital. J Med Assoc Thai. 1995;78(11):618–23.
39 O’Cathain A, Murphy E, Nicholl J. Why, and how, mixed methods research is undertaken in health services research in England: a mixed methods study. BMC Health Serv Res. 2007;7:85.
40 Mazzocco K, Petitti DB, Fong KT, Bonacum D, Brookey J, Graham S, et al. Surgical team behaviors and patient outcomes. Am J Surg. 2009;197(5):678–85.
41 Rafferty AM, Ball J, Aiken LH. Are teamwork and professional autonomy compatible, and do they result in improved hospital care? Qual Health Care. 2001;10(Suppl 2):ii32-7.
42 Firth-Cozens J. Cultures for improving patient safety through learning: the role of teamwork. Qual Health Care. 2001;10(Suppl 2):ii26-31.
43 Davies C. Getting health professionals to work together. BMJ. 2000;320(7241):1021–2.
44 Schmalenberg C, Kramer M, King CR, Krugman M, Lund C, Poduska D, et al. Excellence through evidence: securing collegial/collaborative nurse-physician relationships, part 1. J Nurs Adm. 2005;35(10):450–8.
45 Zwarenstein M, Reeves S, Russell A, Kenaszchuk C, Conn LG, Miller KL, et al. Structuring communication relationships for interprofessional teamwork (SCRIPT): a cluster randomized controlled trial. Trials. 2007;8:23.
46 Zwar N, Hermiz O, Hasan I, Comino E, Middleton S, Vagholkar S, et al. A cluster randomised controlled trial of nurse and GP partnership for care of chronic obstructive pulmonary disease. BMC Pulm Med. 2008;8:8.
No funding. No conflict of interest.